Overthinking female chronic pain: how I’m playing the socially constructed role of a sensible endometriosis patient.
Chronic pain is boring. Nobody wants to constantly hear about the same thing over and over again. How can you re-tell the story of your uterus in both an exciting and convincing way? As a chronically ill female patient, is it your responsibility to share information efficiently — without sounding hysterical or emotional? Could playing the role of a nice and well-behaved patient, improve your chances of getting better treatment?

As an endometriosis fighter, I have been asking these questions over the last few years. My situation is particularly complicated as I’m not only a female patient, but a migrant living in the post Brexit Britain and regularly using the NHS services — feeling extremely guilty about the ‘£350 million’ you keep sending to EU. Additionally, I’m one of those Polish patients, who apparently often annoy NHS staff for doing too much ‘googling’ before their appointments.
As you can imagine, loads of acting to do during my medical appointments. As I’m discussing my pain, I don’t allow myself to be too emotional. I am keen to be super organised with my notes and sound like an informed (but not overly-informed) patient. As silly as this sounds, I’m certainly not alone doing this amount of overthinking and acting.
To understand the emotional labour of an overly-sensitive chronically ill patient like myself, I’d recommend listening to Lena Dunham’s Podcast “Women of the Hour” episode called Sickness & Health. As an experienced endometriosis patient and a badass feminist, Lena perceives herself through the lens of those less-educated doctors as ‘a fucking outrageous bitch with irrational periods’.
Endometriosis is a feminist issue — the condition has been ruining women’s lives for centuries, yet it is still under-researched and poorly understood.
“We don’t know for sure how or why it starts, but we understand something about its mechanism. The endometrium is the tissue that lines the womb, which is shed each month if there is no pregnancy. In endometriosis, these special cells are found elsewhere in the body — mainly in the pelvic area, though they can get just about anywhere. Each month, wherever they are, they obey their nature and bleed. The big three symptoms — of which all GPs should be aware — are painful menstruation, painful sex, and infertility”
Hilary Mantel (Guardian, 2015)
Note: Endometriosis is by definition, when cells similar to those of the lining of the uterus (womb) are found elsewhere in the body.

My-bloody-bleeding adventures started at the age of 12. The excessive bleeding lasted for days, weeks and later months. As a young girl, I had to organise my life around pain and doctor’s appointments. At the age of 13, I was no longer able to do any sports. When saying goodbye to my youth basketball, one of the coaches tried to cheer me up by saying:
“oh, you know, female basketball players struggle to give birth anyway, so you better stop doing sports anyhow”.
According to most gynaecologists, the type of tortures that I was going through, were ‘normal’. Over the years, I have also been repeatedly told that the pain is ‘just in my head’ and that I should simply get used to it, and that things will get better, once I get pregnant.
You might wonder — has anyone ever asked her if she had even considered being a mother back then? The answer is simple: no.
13 years later, in 2014, I was diagnosed with Endometriosis. At first, I was super relieved to find out that my pain was real. However, after a little bit of research, I realised that — in reality — I am still in quite a lot of trouble…
In 2018, it still takes an average of 7.5 years to receive a diagnosis. This means that symptoms such as period pains, nausea, back pain, leg pain, fatigue, pelvic pain, bloating, excessive bleeding, painful sexual intercourse (and many others) might be dismissed as ‘normal’ or misdiagnosed for several years, before you are even considered for a referral to see a correct specialist. There is no known cure for endometriosis.
It appears that “for hundreds of years, pain in menstruating women has not qualified as a medical mystery worthy of actually solving” (Dusenbery, 2018).

In my view, the “menstrual etiquette” stops us from having open conversations about the real social impact of women’s health mistreatment. Talking about, what De Beauvoir described as — ‘bloody mass seeping out’ — of your vagina, might not sound like a pleasant topic to discuss around a dinner table, but it could certainly be an interesting one. In fact, I have tested it myself on several occasions and so far, most of my male friends were always up for a healthy dose of informative period chat.
In order to have our menstrual health taken seriously by society, researchers and the medical community, it is essential to normalise everyday conversations about women’s health and the content of our vaginas. In light of the recent survey by WaterAid on the lack of period knowledge in the UK, these conversations seem to be way overdue.
About a third of women would not feel comfortable talking about their menstrual cycle at all with anyone. As a clear illustration of the taboos that still surround periods also in the UK, more than 1 in 5 women in a relationship feel uncomfortable talking to their partner about period pain (22%), PMT (23%) or their period flow (25%). Around one in six would not even feel comfortable talking to their doctor about issues related to menstruation. This is not surprising, since many women still receive derogatory comments related to their periods, with the most common remark being told they must have PMT when considered to be moody (35%) topping the list.
Source: https://bit.ly/2L6larZ
It is clear that endometriosis is a social justice issue (see more Peterson, 2017) and should be high on the feminist agenda. If you get a chance, take a quick look at the endometriosis online community to learn about the amount of desperation, pain, sadness and anger you can find under hashtags such as endosisters, endopain, endosucks, and endolife.
Many endo-sisters worldwide — despite acting out their female patient role still experience unfair treatment, misogyny or patronising attitudes from medical staff. Their experiences are posted online on a daily basis, among questions linked to the emotional labour such as: how to ask your doctors for extra care, information, how to take more of their time or how to kindly indicate that your current treatment is not working and so on. The digital community, is always there to support one another and I have benefited it from it myself enormously.
However, there are also these critical situations, where there is no time to rehearse your patient — doctor appointment. The times when pain is so real that all you want to do is tell them how it really is, scream and demand medical support.
In June 2017, Alison Kimberley was desperate to get relief for her endometriosis pain at a hospital in Australia. However, her calls for help were dismissed across the hospital before she was told to ‘go home and deal with it’. She did not get any meaningful help and was left distressed and in pain. Her story was similar to so many other endo-sisters.
Kimberley was in severe pain and demanded medical support. She broke out of the nice female patient role and turned into a fighter who fought for her life, health and voices of other female patients. She cried, screamed and demanded help. Nevertheless, her pain was still dismissed.
The problem of the mistreatment of women by the medical system is not only affecting the endometriosis community. In fact, simply being born as a female has a huge impact on the amount of time it will take for you to get a diagnosis. In her recent book “Doing Harm”, Maya Dusenbery provides an in-depth analysis of how women’s pain has been systematically under-researched, ignored and dismissed as hysteria for centuries. On her website we can read the following description of the book:
Doing Harm explores the deep, systemic problems that underlie women’s experiences of feeling dismissed by the medical system. Women have been discharged from the emergency room mid-heart attack with a prescription for anti-anxiety meds, while others with autoimmune diseases have been labelled “chronic complainers” for years before being properly diagnosed.
Women with endometriosis have been told they are just overreacting to “normal” menstrual cramps, while still others have “contested” illnesses like chronic fatigue syndrome and fibromyalgia that, dogged by psychosomatic suspicions, have yet to be fully accepted as “real” diseases by the whole of the profession.‘
In her article for the BBC, she writes that:
A 2013 study concluded that more than twice as many women as men had to make more than three visits to a primary care doctor in the UK before getting referred to a specialist for suspected bladder cancer. So did nearly twice as many with renal cancer. (BBC Article)
Interestingly, Dusenbery, indicates that this type of “gender-biased diagnosing” was published in medical education journals. There is an example of a gynaecology text from 1971, which argued that “many woman, wittingly or unwittingly, exaggerate the severity of their complaints to gratify neurotic desires (2018, p.75). Elsewhere, scholars argued that “women’s illnesses are assumed psychosomatic until proven otherwise”(2018, p.75).
With this amount of data suggesting that female pain is being taken less seriously by some medical professionals, I began to wonder if there was anything I could do to improve not only my situation as a patient but to bring more attention to the problem on a wider scale. On the one hand, I’m keen to get my health under control — thus, I should selfishly play my sensible patient role well, right? To support my theory, I managed to gather some evidence from Dusenbery’s book, who writes that doctors are likely to believe you more if you:
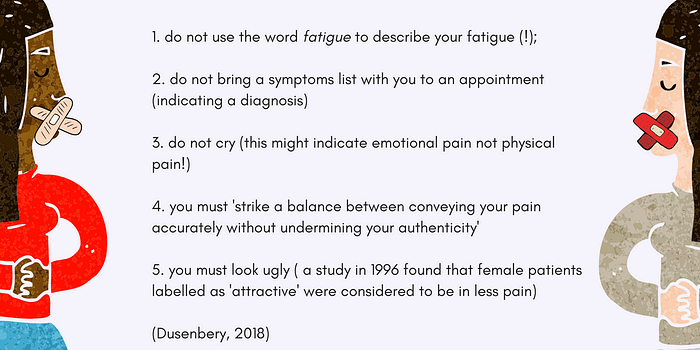
On the other hand, I want to free myself from this absurd role of the nice female (migrant) patient that I adopted so easily — which involves pretending to not know very much (while spending hours on endo forums) and appreciating every second of help from the doctor, and crying in the loo afterwards — where no one sees you…
My feminist voice inside of me is screaming. Not only because I can’t often finish my sentence without being interrupted while discussing my pain, but because endometriosis and women’s health issues have been systematically ignored for years.

Here I’m, in 2018–20 years after I got my first period and heard my first gynaecologist telling me that pregnancy would fix ‘all of this bleeding nonsense’. So many years have passed, not much has changed in terms of endometriosis treatment. In fact, some of the medical fairy-tales are still around.
Last year, I went to see a doctor to discuss my endometriosis symptoms. To cheer me up, the specialist told me something I have heard again and again — ‘don’t worry hun, your endometriosis gets cured once you get pregnant*’.
What was my reaction? I played my female-patient role well. I agreed, left and allowed myself to be emotional later that day.
*Pregnancy doesn’t ‘cure’ endometriosis: more info.







